I donated “Lefty” a year ago today, 11/22/2016, and I am still alive, ready to celebrate! Rob and I are in Thailand today, 1 day ahead of the US, so technically we are celebrating Lefty’s departure 1 day short of a year but on the correct date. 🙂 Thailand is one of my favorite places, so the plan is to go SCUBA diving all day and then have good Thai beer and curry for dinner, and fit a Thai massage in on the beach at some point. It doesn’t get much better than that for us!
I had my 1 year check-in a few weeks ago, and all of my numbers are perfect, meaning, 1 kidney is doing the work of 2 with no problems, and it likely doubled in size this year and is a “super kidney.” I feel 100% and no different than this time last year.
Soooo, what’s next?
I would like to see a conscious effort to change the language we use when we talk about organ donation. Have you ever heard someone say “there is a shortage of organs, 23 people die each day waiting for an organ?” That’s a statement comes from a place of scarcity! The “shortage” is nothing more than a perception. There are millions of people just like me walking around with the ability and willingness to donate an organ while they are alive. The possibility just isn’t in their awareness yet. Do you see? There is not a shortage of organs, there is a SURPLUS of organs, enough for everybody that needs one. My mission is to bring the concept of an organ surplus into society’s consciousness. In addressing the surplus of organs out there (versus the shortage), I believe we can create the opportunity for people to give big and operate from a place of opportunity and possibility. It feels good to give big, and it feels good to be the solution to the problem. We all innately want that, and this act of service to another human is a game changer, what an amazing way to experience purpose! The ripple effect of this kindness has the ability to change the world that we live in. Let’s choose abundance, choose service, and be kind.
The next step is getting onto the speaking circuit with my dad. We have a family story that if told with passion, can help other people. We are seizing the opportunity to create a legacy together! We went to Mikki Williams Speaking School together and have started crafting our story which will eventually be a Ted Talk. We are having fun doing this together, and while we have a lot of work to do, we will rock it. It’s going to be amazing.
Thanks for reading! Call me if you want to donate your parts at 312.927.7655, and email me if you would like to be a guest blogger covering any transplant topic at laurie@swiftpassport.com.
Wow, this was an amazing week, one of the busiest weeks of my life- I have no clean clothes and haven’t unpacked from my weekend travels! But it’s been a memorable and amazing week filled with love, excitement, growth, gratitude, laughter, new and old friends, family, Rob, and unsolved mysteries being solved! I’ve slept in 4 different beds this week in 3 different states, but that’s not what this 6-way is about (fortunately/unfortunately? You can decide that on your own).
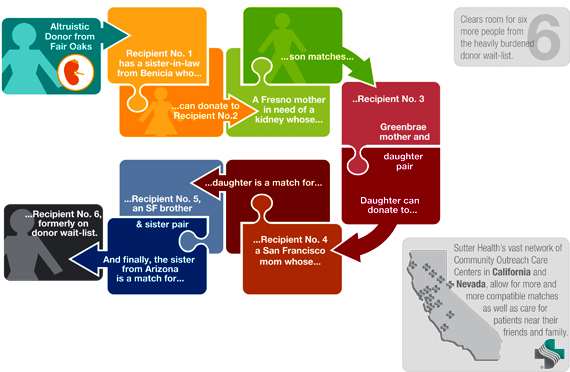
It’s been 7 months since I donated, and the last I heard about what happened after my kidney flew to TX was back in January. That’s when I learned that the chain was at least 3 transplants long and still going. Well this week, I heard confirmation from the Transplant Team that my chain is ended and was 6 transplants long!
So this is what that looks like (with other peoples names, this isn’t my chain)…..
The knowing of something, anything, about the details has been amazing to learn, it just helps me visualize what actually happened. There’s a start and an end to the physical part of the journey, and now I can picture my kidney family. So who are they? There’s me, I kicked it off. Then there are 6 sick people who were in need of a kidney, 5 who had loved ones who wanted to donate to them but couldn’t, so they donated forward so that their loved one could get a kidney from somebody else. How fucking cool is that?! It’s phenomenal knowing the extent of the energetic connection I have with this group of 12 people, who I will forever be connected to, and may never lie eyes upon. It’s just beautiful and it fills my heart with joy. I can’t begin to describe the feeling….
Some clarity that came to me this week that I am excited about is that I want to speak about my experience professionally, and do that with my dad. We are each others biggest fans, and will have fun with this. One day we will do a Ted Talk about this (hear that universe?!). It doesn’t even need to be about kidneys, depending on the audience, it can be about the fact that if you have 2 of something, you should give one away. And feel fucking phenomenal about it!
There are no windows in the rooms where I work. My view is the insides peoples’ bodies; I’m a surgical technician and I work elbow to elbow with surgeons. My job is to prepare the sterile field, that is, to get all the instruments and suture ready to pass to the surgeons. I even work with high-tech robots initially designed for NASA and computer navigation systems that target tissue with great precision.
I work at a large university hospital. It’s phenomenally different from day surgery where people go for things like hernia repairs and total hip replacements and appendectomies. We’re not trauma I, so we don’t see gun-shot victims or car accident victims. Our people range from fairly sick (cancer) to chronically sick (diabetes) or acutely sick to verge the death (ruptured major vessels; organ failure). I’ve seen billions, maybe trillions, of cancer cells. In prostates, breasts, uteruses, bladders, necks, brains, inside throats and lungs and intestines, and on kidneys, livers and pancreases. The surgeons I work with do extensive research– looking for patterns, looking for breakthroughs, looking for cures. They bring fellows and residents and medical students to the OR to train them to be the future generations of super-heroes to fight cancer.
Cancer is even more mysterious when you see and touch it in muscles, bones, organs. Tumors in organs like the prostate can be hard as a rock. A tiny tumor in the breast can represent (but not necessarily) more danger than an enormous one elsewhere. Who doesn’t know someone whose had breast or prostate cancer? Most of us have faces of people we know and love to attach with cancer treatment. I’ve seen cancer look like mucous. There can be literally gallons of mucinous gel in an abdomen with appendicle cancer. It’s as shocking as it sounds to see, and the person has on average, one to five more years to live. We win some battles, increase life-spans and health, but there are times it’s an uphill battle at best, and palliative care is all we shoot for.
For me, I meet patients very briefly, they are on sedative drugs already, just before they go to sleep, while my compassion and fears triggered, I have it easier than the nurses who visit with patients and families before coming to the operating room. Surgeons have it tough and floor nurses have it the toughest. People without cancer have some instinctive, personal, defensive shield when facing those who do, but it does make an impact when you work every day looking at and cutting out cancer.
There is, in this cancer-filled environment, an incredibly bright side to my university hospital. Transplant. An organ transplant can completely turn a life around. A person whose days are numbered, gets a chance to live and feel better again, usually for the first time in many, many years. Not instantly and not always, but almost always. The families and friends of those who’ve passed away and donated organs, know the depth of grief with their loss, and the height of love and pride from the new life that’s generated from their loved ones’ donation. Transplant is often compared to rebirth.
The happiest surgeries for me are putting in organs. The general public is familiar with deceased organ donation. (Most aren’t aware that only five percent of those organs make it to implantation.) A far less familiar form of organ donation is by living donors. It is tremendously moving to meet a living donor who rolls into the operating room to give a kidney or part of a liver to someone. The living donor could be family, a friend, a co-worker, or a total stranger. The donor is scared. Excited. Nervous about what will happen. Afraid of the pain when they wake up. People who are willing to undergo major surgery and risk their own health to improve someone else’s health is about as personal and as sacrificing and frankly, as odd, as it gets. The range of responses from the general public (on the outside of the transplant world) about living organ donation runs the full gamut- from hero worship, to thinking those people are insane, to near revulsion. For the public who briefly considers and weighs living donation, these responses are fleeting thoughts. The realities for living donors of what donation means goes much deeper and lasts forever, for any and all, good and bad, outcomes.
Before I worked in kidney, liver, and pancreas transplant, I didn’t know what a healthy kidney looked like. It might sound funny, but it is so beautiful and perfect. And almost everyone has two and can live just fine with just one! The healthiest patients I see are living organ donors. And they aren’t all in their twenties and thirties- they can be in their forties, fifties, even in their sixties, if they are in good enough shape. Even so, there’s more to the story if someone surgically donates one, figuring he or she will be just the same with the remaining kidney. More physically, emotionally, socially, financially.
More than a decade after working in transplant, when a healthy kidney, especially one from a living donor, is put into a person with end-stage renal disease, it is like Christmas. With 120,000 people on the list for a kidney in the US, one person an hour dies every day, waiting.
For the kidney transplant surgeries, the donor is in a room adjacent to the recipient. The surgeon who takes out the organ of the donor literally walks it (safely!) right next door to the surgeon who is going to put it into the recipient. When I’m the surgical technician in the donor’s operating room and the kidney first comes out of the donor’s body, we have a large bowl filled with ice and solutions to preserve the bright healthy organ. The surgeon takes the solutions and flushes all of the blood out, and inspects the renal artery, vein, and the ureter. When the kidney is flushed free of blood and sitting on ice, it is white. Like a navy bean. The kidney is carried in a basin into the OR right next door.
When I’m in the recipient’s room, I have ice too. The kidney has to stay cold until it is in its new home. When the surgeons have the sick person’s iliac vessels all cleaned off and ready to house the new kidney, I give the surgeons all the sutures to sew the artery and vein of the new kidney there. Just before they sew it they have to clamp off the blood in the vessels of the sick person. That way, the surgeons can see clearly how to sew those pipe pieces perfectly. Once they are sewn together and the new kidney rests perfectly in its new nest, the clamps are taken off. The blood flows into the new kidney, and it goes dramatically from white (navy bean) to red (kidney bean J), and begins to work immediately. The new ureter on the new kidney will have pee coming out in a matter of minutes! We can see it because we haven’t connected it to the bladder yet.
After a few years working in transplant I decided I wanted to give someone one of my kidneys. I went through a rigorous evaluation process. I was turned down due to a history of depression. I had surgery when I was a teenager and know a bit about how the physical impact of surgery almost automatically brings a person down. It’s a brutal blow to the body to be sliced open, the innards rearranged, something originally meant to be there as part of the body’s whole system of working mechanics is shockingly removed, the near-by pieces put back in, no longer in their normal positions, and the layers of tissue and muscle that have been cut through are stitched back together. Really, it’s incredible that a body can withstand all that, and even have a chance to heal up and run just as well as or better than before.
I knew from my ovarian cyst removal that my body was not the same again. I developed adhesions and when I jogged for a certain while, my lower abdomen hurt. It wasn’t until I began working in surgery that I could imagine scar tissue that had grown on the walls of my abdomen pulling and causing sensation that didn’t used to be there. Not a huge deal, but my body is different, and it is because of surgery.
Imagine for living donors, when an organ is taken out to boot, and the body is expected to return to its original state. Things don’t happen that way. Over the ten years I’ve worked in transplant, it’s become a huge desire of mine to keep these amazing people, living donors, in the great health they roll into my OR with. I’ve begun volunteer fundraising for a nonprofit that strives to help living donors with anything they need help with from the point of donation and through the rest of their lives. Living donors need support. No one “makes” living donors donate- yet, if a loved one is suffering and may die, that’s a lot of motivation to want to help. A lot of the community focus is about the sick person who needs to the organ. Someone who donates, who is healthy, can feel like their needs go to the wayside. Especially if things don’t go ideally and health problems occur for donors after donation.
Living donors go through a huge evaluation process, but no matter how much a person learns before-hand, it will never fully prepare anyone for what the donation reality becomes for each individual. It is emotionally, physically, financially, and socially, a complex and transformative experience. From my vantage point of working in transplant I see living donors and recipients as being bonded by a near-death experience and a life-after-near-death experience. They’ve gone to an indescribable place, met, and come back together. Imagine sitting on a couch next to someone you love who has one of your kidneys, and you’re watching Saturday Night Live, laughing at Alec Baldwin, just enjoying the moment. Sometimes it occurs to you that your kidney is in that person you’re with, and sometimes not. But there’s no getting around that all the moments now, consciously or not, are connected between the two of you. My room with no view has given me a perspective on life that no window could have provided.
ABOUT Anne:
Anne Zerby lives in White Bear Lake, MN with her husband. She is a volunteer fundraiser for American Living Organ Donor Fund and works as a surgical technician at the University of Minnesota Hospital, M Health.
Spirituality and religious views are diverse and plentiful in American society. No matter what your particular view, most people have some sense that life does not end when the human body takes it’s final breath. Science does prove to us that you cannot kill or destroy energy, is only turns into some other form. Therein resides the source of speculation and debate.
For sake of this offering, I am sharing a perspective on kidney donation from the idea of karmic implications. Most of us have some idea that what we do impacts future events. We try to be thoughtful, careful and smart with our choices. We may even say “what comes around goes around.” Or “do unto others as you would have them do unto you.” The term karma has origins in eastern religious traditions and essentially means the sum total of your contributions or debits to date. Your karmic condition is where you are at this moment in time based upon the life you are living, or the lives you have lived.
From a karmic perspective the reason a person donates a kidney has karmic origins. Perhaps you owed a kindness of significant proportion or you left a debt unpaid at some point in your existence. Perhaps in this life or another life time you were rescued and your life was saved, and you are paying forward the generosity you received. You are sustaining life, and potentially impacting an entire tribe of people from the inevitable loss that would occur without the donation.
Karma says balance will always be restored. Until it is restored we continue to have experiences that will force equitability. If you have found yourself in a position of donating a kidney, you are supposed to do so. It is part of your karma. Whether or not a kindness was bestowed upon you, perhaps you have a different karma to be of service in a selfless manner. Perhaps you were not selfless in another lifetime or experience, and this is a manner in which you can equalize the karma of selfishness. Or, perhaps you are on the way to becoming an enlightened being, and you simply want to maximize your energetic potential and be an instrument of service. This would generate a karmic implication of significant positive impact.
Where ever you fall in the spectrum of the creation of karmic balance or influence, kidney donation is a selfless and generous act. It often is performed with anonymity. Anonymity is the highest and most powerful form of giving that exists. Kidney donation is a huge boost karmically to anyone who decides to give that gift. In the act you put your own life at peril. No matter how safe the procedure, no surgery is guaranteed to go off without a hitch. You give to someone you may not even know or ever meet, or ever receive a “thank you” from. For those of you have given a kidney, know that you have influenced karma in a very powerful way for yourself, as well as for your recipient.
To those who receive a kidney, this is their opportunity to honor the loving nature of a divine consciousness who seeks to heal and love. They have been given an opportunity to live in an enlightened state of being because they were gifted. It will forever be written on the slate of who they are that by the grace of God, a gift was bestowed upon them. That will impact their psyche, their life, and the life of their loved ones, forever.
The message here is that karma is a reality of living. Until all our karma is resolved we continue to live, grow and having experiences of all kinds. Kidney donors are stacking the deck in their favor by selfless acts of generosity. Kidney donors are executing God’s work. Some might even call you Angels. There is divine activity at play, living large in these scenarios no matter how you shape them.
The only thing left to say to a kidney donor is Thank you. The only thing left for the kidney donor to do is to acknowledge to themselves that they been an instrument of divine intervention. That is an honor bestowed on to a few. Many kidney donors do not want to pat themselves on the back. It’s appropriate to acknowledge that you have been an instrument of divine blessing in another person’s existence. That itself is an honor.
You are good people. You are angels on earth. That is a spiritual truth.
With love and appreciation,
Phyllis King
ABOUT PHYLLIS:
Lovingly known as The Common-Sense Psychic. Phyllis King has worked with tens of thousands of people in 25 different countries. She is known for her practical and down to earth approach. She has been featured on, ABC, CBS and NBC TV, radio programs across the country, and has been published in over 70 print and online publications. Phyllis holds a B.A. in Sociology.
Mentorship, Advocacy and Intuitive Services
Author of The Energy of Abundance, Practical Advice and Spiritual Wisdom to Achieve Anything www.phyllisking.com
Laurie: Hi Kevin, thanks for letting me interview you about health insurance as it relates to organ donors. A lot of donors out there are worried that having 1 kidney will be considered a “pre-existing condition,” with the new healthcare changes.
Kevin: No problem Laurie. I want to start by saying that I have not read through the entire bill that was passed, but I have had some conversations with my General Agent concerning the individual markets and what may be in store. Let’s start with a few things that MIGHT happen.
First, the penalty for not having insurance will be removed. No longer will individuals be “forced” to purchase insurance. However, if you are uninsured for more than 63 days, insurance carriers may charge a 30% late enrollment fee AND, depending on the state, the applicant may be underwritten based on health status.
Laurie: What does underwritten based on health status mean exactly? I don’t speak insurance…
Kevin: underwritten based on health status mean that the insurance carriers may take into account your past medical history to determine the rate at which you will pay for the insurance. Currently, carriers are not allowed to use your past medical history in determining rates. States may petition to increase the age ration on pricing from the current 3:1 ratio to 5:1. Currently, someone 64 years of age cannot be charged more than 3X the cost of someone who is 26 in the same area.
Laurie: Can you give an example of that?
Kevin: Yes… say the monthly rate for someone 26 years of age living in zip code 60622 is $350/month for a particular policy. Under the current laws, that same plan for someone 64 years of age could not cost more than $1050. Under the new law, carriers may charge up to $1750 if the ratio moves to 5:1.
They may also Petition to use a health status factor instead of the late enrollment penalty.
Laurie: what is health status factor?
Kevin: This means that the insurance carriers can take into account your past medical history when determining rates. If they deem you “uninsurable”, you would be forced into the states “high-risk” pool. They may also enact their own state sanctioned essential health benefits, eliminating the 10 essential health benefits currently set up under the Affordable Care Act.
Waivers would require the state to set up a separate high-risk pool for those with pre-existing conditions and this state based pool would receive federal funding. Similar to the old I-CHIPS system Illinois had in place before the ACA.
Laurie: Okay, so this is the big one everyone is really worried about right? Being put in the pool of individuals with pre-existing constitutions and having high insurance rates?
Kevin: Exactly!! Prior to the Affordable Care Act, states had these high risk pools where individuals previously denied coverage could apply for insurance. However, rates were extremely high and many people with pre-existing conditions could not afford the pricing of these plans. I see similar issues if we were to go back to this system. The high risk pools were inefficient, extremely burdensome to enroll in coverage, expensive, and sometimes individuals were placed on waiting lists.
Subsidies are important too. Cost-sharing reductions and subsidies to help lower income families would no longer exist. Under the new law, individuals would be given a fixed dollar amount to purchase coverage. The tax credits would start to phase out for those earning over $75,000, $150,000 for families. The credit would NOT be available to individuals who have access to employer based plans.
Laurie: So what about this is problematic? Low income families who have pre-existing conditions are screwed? And if your employer offers a plan, you are forced to use it pretty much?
Kevin: Correct- the individuals and families with pre-existing conditions and who have benefited the most since the Affordable Care Act was passed would be penalized. I’m not saying that the ACA has been good for everyone, because it has not. It penalizes families who are in good health, forced maternity coverage on everyone, and forced carriers to charge much higher premiums while limiting access to certain providers.
Before the ACA was passed, individual insurance was always much cheaper than company sponsored plans, especially those with 50 or fewer employees. Groups over 50 employees are already rated based on the health of the company. For groups under 50, employer based plans were guaranteed issue-meaning anyone with a pre-existing condition was covered. However, the carriers were allowed to rate the group according to the health of its employees. Groups with a lot of pre-existing conditions were greatly affected by this because everyone was guaranteed coverage. The ACA stopped this practice of underwriting groups under 50 and everyone was age-rated based on where the company was located. If the ACA is repealed, carriers may again start to underwrite for groups under 50, greatly increasing the price to insure employees.
In summary, if passed, the individual insurance market will be changing once again. Concerns about pre-existing conditions are real, and based on our knowledge of the insurance industry, we expect premiums to continue to soar, especially for those with pre-existing conditions. Another major concern among clients is the lack of access to quality providers. Over the last three years, insurance carriers have been dramatically reducing their network of providers, thereby limiting an individual’s ability to seek quality care. It remains to be seen how this will change under the new law, if at all. My early assessment is that the news is not good for individuals with pre-existing conditions, middle income earners who will no longer qualify for cost-sharing, and individuals over 50.
Laurie: So how will this effect me- I am in good health, don’t have a lot of risk factors, but have 1 kidney. Having 1 kidney has not made me less healthy, there is nothing wrong with me. Will organ donation be considered a “pre-existing condition?”
Kevin: Here are the most common “pre-existing” conditions that insurance carriers used to look at. Please note that this is not a comprehensive list and each carrier was allowed to pick and choose what they consider pre-existing. In my opinion, I believe the insurance carriers would look at having 1 kidney as a pre-existing condition. This would make it much more difficult for those to get insurance. Over the course of the next few months, I will have a much firmer grasp on the new law and how it is going to affect our clients. In my opinion, it will be very hard for insurance carriers to change their model for 2018 even if this bill is passed. I believe 2019 is the earliest we could see major changes. How are you feeling about this?
Well, I know I want to pay attention to what is going on, and do what I can to be part of a solution. This isn’t just about organ donors, it’s about a lot more than just this particular group of people- I mean RAPE is actually listed as a pre-existing condition, that’s just messed up. There is a potential long term financial expense that I have to think about now which is inconvenient. I think the worst part is that this will detract people from wanting to be an organ donor. It changes the act of organ donation from a short term commitment to a long term commitment with unknown financial risks.
All things considered, I would donate again. It’s just interesting that when I made the choice I felt much more protected than I do now with these pending healthcare changes. NM makes it clear that these things CAN change, I knew the risk. I just didn’t think I would have to worry about it.
Readers, I invite you to comment if you have more information on this topic!
Thanks again Kevin!
ABOUT KEVIN:
Kevin attended Illinois State University. Kevin was a commodities trader on the floor of the CME for 15 years before entering the insurance industry in 2012. Chris Felix, owner of Gizmo Health Insurance, was his old trading partner and started Gizmo in 2007. Kevin came on board in June of 2012 and they have been a two man shop since. They specialize in helping individuals and small business owners navigate the confusing world of health insurance.
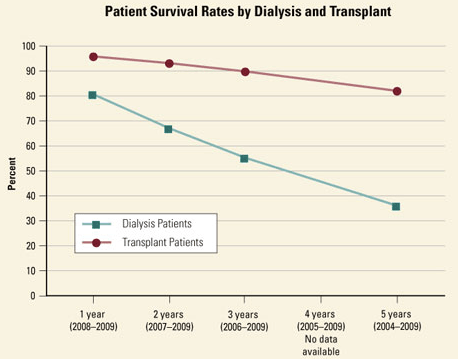
One of the greatest things about being a kidney donor is that by donating your kidney, you can prevent somebody with kidney disease from ever having to go through dialysis. If you donate a kidney to somebody who is already in dialysis, once they have a healthy kidney they will no longer need dialysis. Dialysis is not a long term solution to cure kidney disease, but transplant IS a long term solution in most cases. This graph shows the survival rates of dialysis patients and transplant patients side by side.
“Dialysis patients have a 25% chance of death after being on dialysis for one year; their chance of death increases to 65% after five years. Although dialysis extends patients’ lives, it comes with a large swath of side effects that range from anemia and muscle cramps to bone diseases. It’s much better, therefore, to get a kidney transplant, if possible.”
Getting a living donor before your kidney disease progresses to the point where you need dialysis produces the best possible long term outcome. This is because there are better outcomes from kidney transplant when the kidney comes from a living donor vs a deceased donor. Here is a graph from the National Kidney Foundation that illustrates this.
Strangely, this is really easy information to find online, but over and over again, we meet people in the transplant community who don’t understand their options when it comes to deciding between dialysis and transplant. So where is the disconnect?
John Oliver tackles this topic this week on Last Week Tonight, and the information he spotlights, is pretty disturbing. As Oliver explains, “kidney dialysis occurs in centers outside of hospitals, and roughly 70% of these are run by two private, for-profit companies: DaVita and Fresenius. These companies have fairly loose laws about quality control measures. For example, only one nurse and no doctors need to be present at a center at any given time.”
“Companies like DaVita and Fresenius legally have to tell patients that getting themselves on the kidney transplants list is another option, but they’ve built entire business models on keeping as many patients coming through as possible. They don’t do a lot to advertise this other option, and instead —like any self-respecting business—do all they can to maximize their own profits. In 2009, the CEO of DaVita, Kent Thiry, told University of California, Los Angeles business students that “if [he] had 1,400 Taco Bells and 32,000 people who worked in them [he] would be doing all the same stuff.”
If you know somebody with kidney disease who is facing decisions regarding transplant and dialysis, this episode is a must watch! Be your own health advocate. If you won’t, who will?
I have always been a very strong advocate for organ donation. Going back 24 years, when I was 16 years old and I got my driver’s license. I can remember thinking if something was to happen to me, I would want to help someone in need. Since that day, organ donation has been a part of my life in several ways.
Twelve years later, my father suffered a heart attack and stroke that eventually lead to his death. Although they were unable to use his organs for transplant, my siblings and I were given the opportunity to donate my father’s body to science because of the need of cadavers to be used for medical advances.
In 2011 my mother-in-law had a massive stroke that took her life. Once the doctors had informed us that she had lost all brain function, we met with the Gift of Life team and the family made the decision to donate her organs. This gave us all comfort at a very devastating time.
About 4 years ago, my mom was tested to be a living kidney donor for a man that was born with one kidney and was suffering from kidney failure in his other. Thankfully my mom was a match and was able to donate one of her kidneys to him. That selfless act inspired me to want to do the same if I were ever in that situation. I actually tried to see if there was national database that I could be listed on, like the bone marrow registry that I had joined a few years before, but wasn’t ever able to find the information needed.
On April 14, 2016 I was going through my Facebook timeline and came across a flyer that had been shared by one of my friends. As soon as I saw it, I recognized that the person in the pictures was someone that I had been friends with over 20 years ago and she was in need. She had been battling a rare disease of the bile ducts in her liver known as PBC, Primary Biliary Cholangitis. For 10 years her medical team had been managing it through medications, but it came to the point where she was in need of a transplant and a living donor was her best chance.
Kelly and I had gone to the same high school, but it wasn’t until we both started working at the same place that we became friends. Shortly after she started working there, we were practically inseparable for about 2 years. Although we had lost contact throughout the years, I just knew that I had to be tested. Without any hesitation I called Northwestern Hospital. I live with my husband and children in York, PA; however, I was already planning on being in the Chicago area about 2 weeks from then, so they were able to schedule me to be tested while I was there. Two weeks after the testing was done, I got a call that confirmed I was a match.
After it was confirmed I was a match there were still a few things I had to do before they would clear me for surgery. I had to have a biopsy of my liver to test for a fatty liver and I had to lose 20 pounds. I went for the liver biopsy on July 5 and the tests showed that my liver was perfectly healthy. I then started the process of losing weight. By the end of September I had lost the 20 pounds, but I had to go back to Northwestern for another evaluation to ensure I was still healthy enough to go through surgery. That evaluation took place on October 13. When I received the call from the transplant coordinator that I had been cleared for surgery we set the date of surgery for November 30.
I was a ready to go in for my pre-op testing when we got a call that Kelly’s insurance was not going to cover a living donor. This was devastating news. It took about a week or two to get that straightened out, but by then it was too late for us to proceed with surgery on November 30. Our surgery was rescheduled for December 5, with pre-op testing to be done on November 25, the day after Thanksgiving.
On December 5, Kelly and I got to the pre-op holding area and started getting prepped for surgery when we find out that due to 4 emergency transplants over the weekend, they were unable to proceed that morning. Surgery was rescheduled, yet again, for 2 days later.
December 7 was the big day. Although we were anxious and excited, we had a hard time letting ourselves believe that it was finally happening. We got to the pre-op holding area and once we met with the surgeons, we were assured that we were going to proceed.
Both of our surgeries went well, with only a few small complications. I had some scar tissue they had to deal with from when I had my gallbladder removed 3 years prior and it took them a lot longer than anticipated to put the liver into Kelly, but neither of these things caused any lasting problems. Here is me with kiddos, post surgery.
Since I lived out of town, it was required that I stay in the Chicago area for approximately 2 weeks after surgery to ensure that I was healing properly. After being cleared to go home, I flew home on December 19. The next day I was in a considerable amount of pain that was not being relieved by taking Tylenol and I had been off prescription pain medication for 5 days, so I didn’t have anything stronger to take. Hesitantly I went to my local hospital to see if they could do something for the pain.
It was a good thing that I listened to my body and went to get medical attention, because it turned out that I had blood clots in both sides of my lungs. I was immediately admitted to the ICU to begin treatment. Shortly after starting the Heparin, a clot dislodged and went to my heart. This was the scariest feeling ever. I couldn’t breathe, I was sweating profusely and it hurt so badly. Luckily that didn’t happen again. Then, after doing a blood test they realized that my blood platelets had dropped to extremely low numbers. Typically when this happens after starting Heparin it is due to a condition called Heparin Induced Thrombocytopenia, or HITT. They stopped the heparin and tested me for Hitt, but the test came back negative, so they started the Heparin again. For about 3 days they could not figure out why my platelets were so low. On Christmas Day they decided that I needed to be transferred back to Northwestern to be treated by the transplant team.
After I arrived at Northwestern, they decided to retest me for HITT and this time it came back positive. Apparently I had been developing the condition as they were treating me with the Heparin. It took another 15 days in the hospital to get me off the Heparin and switch me to Coumadin.
I just finished my 3 month Coumadin treatment and have had a CT scan and ulatrasound that show that the clots have resolved. It was also determined at my three month post-op checkup that my liver function is back to 100%. I can resume all normal activities, including being able to drink alcohol, with the exception of donating blood – that will have to wait until December.
It is so amazing to look back at everything that has happened in the past year and to think that, I donated part of my liver and am back to normal already. Although we had some setbacks and I encountered such a huge complication, I would still do it again if I were able to. Knowing that I gave someone their life back and allowed them to look forward to a long, healthy life with her family is such a great feeling.
I hope that hearing this doesn’t scare anyone out of wanting to consider living organ donation. I tell my story to inform people of the possibilities of complications and how even if they happen, you do get through them.
Peace, Love and Recycle Yourself,
Rebecca O’Marrah
ABOUT REBECCA:
Rebecca is a living donor who lives in PA with her loving family. She donated a portion of her liver to a high school friend (Kelly Drey) December 2016 after becoming aware of Kelly’s need for a liver on Facebook! If you have any questions about living liver donation or anything Rebecca went through, please feel free to email her at romarrah@gmail.com. She is a fantastic donor advocate with experience to share.
April is Organ Donation Awareness Month, and in the spirit of giving, my friend Kate Griggs and I are starting an annual gathering at The Bean in Millennium Park. Our goal is to get as many organ donors and recipients in one place at the same time. Next year we will shoot to set a world record! To set a world record next year we will need at least 250 donors to show up at the same time. Anybody who supports organ donation is welcome!
We believe organ donation should be cost-neutral, meaning you should never have to decide or not decide to donate based on your financial needs. To support this belief, we are asking for donations to gift to The American Living Organ Donor Fund (ALODF). ALODF is a nonprofit dedicated to fully supporting the American living organ donor to achieve their goal of saving another person’s life. They improve the experience of living organ donors and their loved ones by supporting them through the organ donation journey, through their network of donor patient Navigators who support their lives personally and financially. In 3 years, this group has helped with over 100 transplants.
One of the purposes of this blog is to document the timeline of a kidney donation experience so people considering organ donation have an idea of the time and resources required to get through the experience. Obviously this will vary from person to person and center to center. Through my journey I have gotten to know several other kidney and liver donors, and none of us had the same exact experience. You can check out the detailed blow by blow of my experience on the This is Timed page of the blog.
Broken down, getting approved to donate and being matched was a minimal time commitment (36 hours) stretched over 8 months. After surgery I was pretty useless for 2 weeks. The third week I didn’t feel great, but could work 1/2 days at work. I had one extremely rough day during week 3 where the pain peaked, and spent one night back at the hospital. Week 4-6, I felt great other than needing a little extra sleep. By week 7-8 I felt completely back to my old self, and my vitality had completely returned. It was a major focus of my life and energy for 10 months from the time I decided to do it, till the time the donation was over, and I felt back to my old self. Not bad! This week I am 11 weeks out from surgery, and feel awesome. I think I actually feel better than I did before the donation!
If you are trying to figure out how this timetable will translate into your donation experience, it’s a great idea to talk to multiple donors. Don’t make the mistake that I did and assume that your recovery will be on the short end of the spectrum, because you are superwoman. That sets you up for disappointment if you don’t hit the benchmarks in your head. Figure out what you need to do to be patient with your body during recovery, and just give your body what it needs when it needs it! Walk as much as you can and water the bean all day. Plan for a long and slow recovery, and then be pleasantly surprised if it goes a little faster than expected!
Please contact me if you would like to be connected with other kidney or liver donors to see how their donation timeline compared to mine. There are tons of donors out there who would love to talk to you, including me! If you are a kidney or liver donor, I would love it if you would comment about your donation experience so that our readers can see what the experience is like for multiple donors. If you are open to being contacted, feel free to post your contact information as well. Thanks in advance!
This past Thursday marked the 1 month anniversary of my kidney donation. I would say I am at 87%, my only complaint is that I get tired easily. If I could sleep 10 hours a night, I would! In terms of side effects, this one really isn’t so bad, as I have an awesome bed, and am gifted when it comes to the art of sleeping. The hardest part of my recovery was the emotional toll that it took. I felt weepy and emotional, and not like my normal, positive self. I am thrilled to say that today I feel like my old self again! I had a follow-up email from NM on my 1 month anniversary letting me know 3things:
My recipient and their new kidney are doing very well!
My recipient doesn’t want to connect with me yet, and respectfully requested we not check back in for awhile
The chain is so far 3 transplants long, and still going. This means at minimum, the chain will result in 4 transplants.
I would really love the opportunity to connect with my recipient, however this can only happen if the recipient chooses for it to happen. They know I am eager to connect, and the ball is in their court. For me, it would be rewarding and exciting to meet, and it would give me closure. Most people who donate an organ know the recipient. I imagine the recovery process is different for these people- the reward of the donation is right there in front of them. They can see the life they impacted. In many cases they can watch somebody they love dramatically change from being sick to being healthy. It’s a nice reward on the tough recovery days! In my case, I don’t get to see that. Sometimes it feels like I didn’t actually donate a kidney. I respect the recipient’s privacy even if I don’t understand it. Confirmation from NM that the recipient is healthy, and knowing that the chain is still going makes me happy, and makes me feel good about donating. I realize I should not have made the assumption we would meet!
An online friend, Diane Brockington, posted this, and while it took a few weeks to resonate, I think she’s right:
“Your reward isn’t delayed-it’s there every time you open your eyes in the morning, close them at night. The gift you gave was the decision to donate. After that, so many factors come into it that are completely out of your hands that you have to focus on the gift. Undiminished by the presence of a thank you. You did it. You gave. Rest in that.”
I had a particularly nice Christmas this year- I spent it with my Dickinson family and we had some really nice quality time together. It was at my house, but my mom did all the work, including making sure we all matched (THANKS MOM)! I am so grateful for all of these guys. They have been so loving and patient with me. Donating a kidney is #thebestideaever, but wow, you can’t do it without a support system. I didn’t fully understand how much my decision to donate would effect those around me. I am glad they were up for it 🙂



 Anne Zerby lives in White Bear Lake, MN with her husband. She is a volunteer fundraiser for
Anne Zerby lives in White Bear Lake, MN with her husband. She is a volunteer fundraiser for 
 Lovingly known as The Common-Sense Psychic. Phyllis King has worked with tens of thousands of people in 25 different countries. She is known for her practical and down to earth approach. She has been featured on, ABC, CBS and NBC TV, radio programs across the country, and has been published in over 70 print and online publications. Phyllis holds a B.A. in Sociology.
Lovingly known as The Common-Sense Psychic. Phyllis King has worked with tens of thousands of people in 25 different countries. She is known for her practical and down to earth approach. She has been featured on, ABC, CBS and NBC TV, radio programs across the country, and has been published in over 70 print and online publications. Phyllis holds a B.A. in Sociology.




 ABOUT REBECCA:
ABOUT REBECCA:
 This past Thursday marked the 1 month anniversary of my kidney donation. I would say I am at 87%, my only complaint is that I get tired easily. If I could sleep 10 hours a night, I would! In terms of side effects, this one really isn’t so bad, as I have an awesome bed, and am gifted when it comes to the art of sleeping. The hardest part of my recovery was the emotional toll that it took. I felt weepy and emotional, and not like my normal, positive self. I am thrilled to say that today I feel like my old self again! I had a follow-up email from NM on my 1 month anniversary letting me know 3things:
This past Thursday marked the 1 month anniversary of my kidney donation. I would say I am at 87%, my only complaint is that I get tired easily. If I could sleep 10 hours a night, I would! In terms of side effects, this one really isn’t so bad, as I have an awesome bed, and am gifted when it comes to the art of sleeping. The hardest part of my recovery was the emotional toll that it took. I felt weepy and emotional, and not like my normal, positive self. I am thrilled to say that today I feel like my old self again! I had a follow-up email from NM on my 1 month anniversary letting me know 3things:
